Jennifer Bauwens, Ph.D.
March 11, 2026
Gender Dysphoria and the Social Transition Intervention
Key Takeaways
« The gender affirming care model (GAC) has been the predominant intervention used to treat gender dysphoria, a mental disorder that occurs when a person has psychological distress about their biological sex.
« The first step of the GAC intervention is called social transition. This step and the entire GAC model has repeatedly shown to lack scientific rigor.
« When children are supported and left to mature without gender affirming care, the majority report a psychological understanding of their identity that matches their biological reality.
« Despite the lack of scientific evidence, mental health clinicians continue to use social transition.
« To further add to the complexities of this issue, there has been a debate in the public discourse about the diagnosis itself and whether it should be characterized as a disorder or a civil rights issue.
« Misunderstanding about the nature of gender dysphoria as a mental disorder has made space for school officials, paraprofessionals, and other non-clinically licensed individuals to use a clinical intervention albeit a discredited one.
« This brief gives reasons why gender dysphoria should remain classified as amental disorder and the reasons for GAC to be recognized as a clinical intervention.
Introduction
Over the last decade, mental health practitioners have increasingly diagnosed minors with gender dysphoria, a psychological disorder used to describe a person’s mental distress about their biological sex. Gender dysphoria was once considered to be a very rare psychological disorder. As the Diagnostic and Statistical Manual (DSM) for Mental Disorders IV-TR stated, “only a very small number of children with Gender Identity Disorder [Gender Dysphoria] will continue to meet criteria for Gender Identity Disorder in adolescence or adulthood” (APA, 2000, p. 579). Today, the ideas contained in this diagnosis are used both formally and informally with much greater frequency than at any time in the history of the diagnostic construct (Bachmann et al., 2024; Sun et al., 2023; Horowitz, 2025).
The rise in diagnoses is disconcerting from the standpoint that more youth are expressing distress about the reality of their biological sex (Rawee et al., 2024). Recent polling shows that roughly 5% of young adults identify as something other than their biological sex (Brown, 2022). What’s more, these numbers translate to a rise in youth undergoing a risky treatment protocol (e.g., Grandview Research, 2020; American Principles Project, 2025) that has been repeatedly shown to be ineffective at best, but growing evidence indicates great harms (e.g., Department of Health and Human Services, 2025b; Cass, 2024; American Principles Project, 2025).
The Dangers of the Social Transition
When these children are supported and left to mature without gender affirming care, the majority report a psychological understanding of their identity that matches their biological reality.
Despite numerous scientific reviews of the literature, the intervention, known as “gender affirming care” (GAC), has recently been endorsed by major professional psychological and medical organizations (i.e., American Psychiatric Association; American Academy of Pediatrics; Endocrine Society) as the treatment of choice for gender dysphoria (e.g., American Academy of Pediatrics, 2018; 2023;American Psychiatric Association, 2026). According to this model, the first step for those with gender dysphoria is to intervene by socially transitioning the person, thereby theoretically reducing psychological distress and helping the person embrace a transgender identity. This includes mostly non-medical interventions such as adopting new pronouns, changing identification cards, using sex-segregated spaces that differ from one’s biological sex, and changing one’s clothing and hair to a more stereotypical presentation that is more consistent with the sex or entity that is the object of their identification. But based on the literature, initiating the social transition part of the GAC model will lead most minors down a path to the most physiologically damaging aspects (i.e., cross-sex hormones, surgeries) of the protocol (Olson et al., 2022; Zucker, 2018).
When these children are supported and left to mature without gender affirming care, the majority report a psychological understanding of their identity that matches their biological reality (Ristori & Steensma, 2016; Singh et al., 2021). To further add to the complexities of this issue, there has been a debate in the public discourse about the diagnosis itself and whether it should be characterized as a disorder or a civil rights issue (Szemanski, 2020).
A Rise in Paraprofessional Use of Social Transition
The lack of clarity about the nature of the diagnosis creates misunderstanding regarding who is allowed to make the determination of gender dysphoria. This lack of clarity has created space for paraprofessionals and non-clinically trained and unlicensed individuals to employ the GAC model, which is a clinical invention. Although the intervention lacks empirical support (e.g., Department of Health and Human Services, 2025b; Cass, 2024), it nonetheless remains a model that is associated with a psychological diagnosis.
As of early 2026, 27 states have enacted legal protections for minors against the physiological steps of the GAC model. Since President Trump began his second term in January 2025, his administration has also pursued protections for minors from these procedures by withholding federal funding to hospitals and public institutions (Exec. Order No. 14187, 2025). Most of the federal efforts and state-wide bans impact the distribution and administration of puberty blockers, cross-sex hormones, and gender-affirming surgeries. Although the U.S. Food and Drug Administration (FDA) recently announced that warning letters were sent to 12 manufacturers and retailers for marketing breast binders to children for the purposes engaging in social transition (HHS, 2025), little has been done to widely address social transition, and only a few states (including South Carolina, Tennessee, and Texas) have enacted protections that address this first step to the GAC intervention. This part of GAC has remained relatively untouched, and yet, this is where the onboarding process begins the most notorious aspects of the intervention.
This brief will outline the problems with the 1) gender dysphoria diagnosis and 2) the problems with social transition, which is the first step to the gender affirming “treatment” protocol. This brief will also highlight the reasons 3) that trained clinicians should not use social transition, and why no school employee or any person working with children should be allowed to employ social transition or any clinical intervention. Policy and research recommendations will follow.
Part 1: Problems with the Gender Dysphoria Diagnosis
Gender Dysphoria Is a Mental Health Disorder
Psychological diagnoses that are contained in the Diagnostic and Statistical Manual for Mental Disorders (DSM) are made by a qualified medical or mental health professional (National Alliance on Mental Illness, 2020). When it comes to diagnosing gender dysphoria—or as it was previously referred to as gender identity disorder (American Psychological Association, 1980)—there has been much confusion over who determines the condition and the nature of the diagnosis itself. Some researchers and proponents of the transgender movement have argued that the gender dysphoria diagnosis should not be included in the DSM because it is a manual that describes and categorizes mental disorders (Stein et al., 2021). To include gender dysphoria in the Diagnostic and Statistical Manual for Mental Disorders necessarily associates the transgender phenomenon with pathology rather than an experience that is indicative of sound mental health. Those who have advocated for removing the diagnosis have argued that the disorder is only in the DSM for the purposes of having an insurance billing code to reimburse gender-affirming care interventions (Bento, 2018).
Gender Dysphoria and Other Disorders
Aside from gender dysphoria’s placement in the DSM, another indication that the diagnosis is a mental health condition is the fact that it is often present with comorbidities and neurological conditions. For example, gender dysphoria often occurs alongside other psychiatric symptoms, exposures to traumatic events, and autism (Frew et al., 2021; Glidden et al., 2016; Van Der Miesen et al., 2016; Kallitsounaki & Williams, 2023). This is further evidenced by the commonly cited claim that minors will commit suicide if gender affirming care is not offered (Hughes et al., 2021). Ongoing expressions of suicidal ideation can be indications of psychiatric issues (Sher, 2023). Notably, suicide risk has been the primary impetus for initiating GAC (Herman et al., 2019), giving more evidence that gender dysphoria and its expressions are characteristic of a mental health disorder.
History of Gender (Biological Sex) Identity Confusion Diagnoses in the DSM
Throughout several iterations of the DSM, the American Psychiatric Association aimed to lessen the pathology associated with the gender dysphoria diagnosis by making several notable changes (Drescher, 2010). However, the original conceptualization of the diagnosis was not separate from the idea of a maladaptive phenomenon.
Early indications of the gender dysphoria diagnosis were formalized in the second iteration of the DSM. At that time, the diagnosis was formulated based on the observations of mostly adult men who were sexually aroused by cross-dressing as women (Blanchard, 1989). The diagnosis later included gender identity and was no longer specific to children (American Psychological Association, 1980). During this iteration, the diagnosis was still considered maladaptive and a disorder. By the fifth iteration of the DSM, the diagnostic term was renamed to exclude the disorder terminology (American Psychiatric Association, 2013).
Despite the lack of clinical evidence, the changes to the DSM happened rather quickly. Below is a list of changes that were made to the gender-related disorder:
Changes to the Diagnosis for Insurance Reimbursement As the list above details, the last two iterations of the DSM were heavily focused on the elusive prospect of reducing stigma rather than on scientific evidence. This is a departure from the way that many other clinical issues in the DSM have been conceptualized (Regier et al., 2013). Tailoring diagnostic criteria to this end ultimately lessens the validity of the diagnostic construct and further calls into question the priority of obtaining gender affirming care at the expense of an accurate patient assessment. The real conundrum with the current status of the diagnosis is that it is unclear whether gender dysphoria is something to celebrate as a fixed trait that exemplifies a healthy psychological state (Cohen et al., 2022) or as a condition to treat with the intent to bring the psyche into alignment with biological reality. The latter, however, has not been the goal of most treatment, research, or intervention development (e.g., Haupt et al., 2020). Because the basic understanding of the gender dysphoria phenomenon is so unclear, the aims and outcomes that the intervention(s) are supposed to address and produce are too. The confusion about gender dysphoria has arguably grown in tandem with the changes that were made to the DSM diagnosis in 2013. Dropping the term “disorder” while leaving the diagnosis in a book for mental disorders did nothing to dispel any misunderstanding that surrounds the gender issue (Drescher, 2025). Similarly, it is problematic to normalize the ideas that undergird the gender dysphoria diagnosis while simultaneously advocating for GAC as “medically necessary treatments” (American Psychiatric Association, 2020). This begs the question, why would psychologically healthy people require a medically necessary treatment that involves intervention? The fact remains, the diagnosis has been used by psychological and medical providers to bill for services to address gender dysphoria, and the diagnosis remains in the Diagnostic and Statistical Manual for Mental Disorders (Drescher, 2025; American Psychiatric Association, 2020). If the gender dysphoria issue is to be considered normal and a non-clinical matter, Bento’s (2018) point should be heeded, and it should be removed from the DSM, a book about mental disorders. |
- DSM II (American Psychiatric Association, 1968): Transvestitism was classified under the category of sexual deviations. The disorder was evidenced by sexual arousal from cross-dressing (Blanchard, 1989).
- DSM III (American Psychiatric Association, 1980): This iteration of the DSM made two changes to the disorder:
- Transvestitism was referred to as transsexualism.
- ‘Gender identity disorder of childhood’ was introduced and included under psychosexual disorders.
- DSM-IV& DSM-IV-TR (American Psychiatric Association, 1994; American Psychiatric Association, 2000): Transvestitism and gender identity disorder were collapsed into one name but with different criteria for adults and adolescents. Gender identity disorder became the new overarching name for both age groups, and the diagnosis was placed under the category of sexual and gender identity disorders.
- DSM-V (American Psychiatric Association, 2013): The diagnosis was no longer associated with the term disorder. The new diagnosis was renamed “gender dysphoria,” and the criteria for the disorder were changed. Three different age groups were added to the disorder, including children, adolescents, and adults. An additional specifier for “post-transition” was added, which was given to recognize the need for continued medical care (i.e., hormones, surgeries).
- DSM-V-TR (American Psychiatric Association, 2022): The language was changed to what was thought to be more inclusive and less stigmatizing. For example, what was once referred to as natal female, is now referred to as “individual assigned female at birth.” Instead of “desired gender,” it is now “experienced gender.”
As outlined above, the DSM-V (American Psychiatric Association, 2013) underwent the most marked changes to the nature of the diagnosis. The DSM-V version of gender identity disorder states that “gender non-conformity is not in itself a mental disorder.” The American Psychiatric Association goes on to say in their statement about the newly minted diagnosis that “discussions continue among advocates and medical professionals about how best to preserve access to gender transition-related health care while also minimizing the degree to which such diagnostic categories stigmatize the very people that physicians are attempting to help.”
The American Psychiatric Association’s statement about best practices also sheds light on their conceptualization of the new diagnostic parameters, which focus on destigmatizing the definition of gender dysphoria. Regarding best practices, they suggest that “gender affirming therapy should be taught to all staff” (American Psychiatric Association, 2017).
Protected Class Status Based on a Mutable Psychological Diagnosis
Still, some who propose that the transgender experience is completely normal have also advocated for those who identify as transgender to be classified as a federally protected class of people (Cohen et al., 2022). The protected class designation gained a lot of traction in the years during the Biden Administration and was reflected in policy changes such as section 1557 of the Affordable Care Act, Title IV and women’s sports, and foster care policies.
The case for the protected class designation was based on how a person thinks and feels about their identity—but thoughts and feelings are mutable and should not be characterized as static traits (Ristori & Steemsma, 2016; Singh et al., 2021). There is a mutable quality to all types of emotions associated with dysphoric symptoms, regardless of whether the person identifies as the opposite sex or something other than their humanity (e.g., the furry phenomenon) (Hsu & Bailey, 2019). To give further evidence that dysphoric symptoms are mutable, we are seeing a growing population of men and women who are desisting or detransitioning from a transgender or a transhuman identity (e.g., “detrans” support websites like r/detrans).
Efforts to assign a protected class designation to those who present characteristics of gender dysphoria only muddles what should only be a clinical issue. To truly be part of a protected class is to suggest that gender dysphoria is a mental health problem that can be characterized as a disability. Yet Congress explicitly rejected this characterization when it excluded “gender identity disorders not resulting from physical impairments” from the Americans with Disabilities Act's (ADA) (2019) definition of disability. When Congress enacted the ADA in 1990 and amended the Rehabilitation Act in 1992, it explicitly excluded “gender identity disorders not resulting from physical impairments” from the statutory definitions of “disability” and “individual with a disability” (29 U.S.C. 705(20)(F)(i); 42 U.S.C. 12211(b)). In December 2025, the Department of Health and Human Services proposed a rule reaffirming this exclusion, clarifying that “gender dysphoria not resulting from physical impairments” is encompassed by the statutory language Congress enacted—regardless of the DSM's 2013 renaming of the diagnosis (90 FR 59478).
Nevertheless, for gender dysphoria to be a disability, it would mean that the person experiences a level of psychological distress that has impaired their ability to function and manage their life (ADA National Network, n.d.). In this case, the aim of treatment should be to expand one’s psychological capacity to function. This is the goal of clinical and case management work with those who are psychologically disabled (American Psychological Association, 2023). Therefore, any intervention should work towards lessening the key features of the disorder and not to further advance the pathology. For example, psychological treatment would never entail withholding food from someone with anorexia nervosa or giving laxatives to someone suffering from bulimia. In the same way, it is illogical to affirm a pathology through a treatment protocol that works to embed the cognitive distortions of the dysphoria or advance the condition in the wrong direction.
Good clinical practice does not affirm pathology by using interventions that aim to further embed the cognitive distortions that undergird dysphoric beliefs and feelings.
Diagnosis, Identity, and Overuse
From a clinical standpoint, making both gender dysphoria and access to gender affirming care into a civil rights issue is a dangerous practice (Wing, 2025). As previously stated, the civil rights argument (apart from a disability) positions the gender dysphoria diagnosis as a mostly fixed or immutable trait. This is how the gender issue was portrayed during the Biden Administration (Morrison, 2022). Advocating for the expressions of gender dysphoria as a civil rights issue is done at the detriment of the patient because this argument conveys that the diagnosis is unchangeable.
When change is possible, that truth should be conveyed, and good clinical practice should aim to resolve or at least ameliorate distress and/or bolster coping skills through proper treatment (when someone is willing). To tell someone that their condition is fixed when it is not is bad practice and can wed a person suffering with distress about their identity to a diagnosis. In this way, a civil rights claim has the potential to further the person’s belief that they are their diagnosis, rather than the reality that they are a person with a condition that can be helped. Again, this proposition is counter to the vast majority of research addressing gender dysphoria in minors, literature of which has shown that the distress can be attenuated and even resolved (Department of Health and Human Services, 2025b).
Mental Illness Identity
Additionally, there is a commonly occurring phenomenon in the psychological fields in which patients incorporate their diagnosis into their identity. Some refer to this as a mental illness identity (Eddington & Badillo-Winard, 2024), and this can happen when the patient has difficulties separating themselves from a diagnosis (Paris, 2021). Having clear and attainable treatment goals can help facilitate an understanding that a person’s identity is not rooted in a diagnosis and that change is possible, whereas characterizing the diagnosis as if the symptoms were fixed creates more opportunity for the diagnosis to become one’s identity (Eddington & Badillo-Winard, 2024; Singh, 2024).
En Vogue and Overused Diagnoses
Another known problem in the psychological field is the tendency for a diagnosis to become trendy. This can happen when a psychological issue becomes the focus of research, education, training, and clinical discourse. While this is not a new issue in the field, it is an important one that can lead to a misdiagnosis and an improper treatment plan. This has been observed in the past, when the psychological profession popularized several diagnoses, such as borderline personality disorder and ADHD (Paris, 2021).
To avoid an inaccurate diagnostic assessment, mental health practitioners need to be aware that their judgment can be subject to cognitive biases like the Baader-Meinhof Phenomenon (i.e., learning about gender dysphoria and subsequently seeing the diagnosis in everyone). Instead, the practitioner should look for evidence to disconfirm their observations, but this is not often practiced. Thus, popular diagnoses can be the source of overuse in the clinical profession. There are numerous indications that the gender dysphoria diagnosis is among the latest cluster of symptoms to be overdiagnosed by the clinical community (e.g., Bachmann et al., 2024). The proclivity for clients to take on the mental illness identity and for practitioners to overuse the gender dysphoria diagnosis are important factors that need to be evaluated with respect to both practice and research.
A Poorly Constructed Diagnosis and a Loosely Crafted Intervention
All the aforementioned factors are highly consequential as they can contribute to an inaccurate assessment, a misdiagnosis and ultimately a misguided treatment plan. Without an accurate assessment, the intervention or treatment will not be properly constructed to target the right issue (Eldh et al., 2017). For example, the harms that can follow a loose approach to diagnosis or poorly defined diagnostic criteria can be readily observed in the medical profession. An undiagnosed cardiovascular issue or misdiagnosed disease can result in a delay in treatment and the possibility that the disease is not contained. This fact is no less true when it comes to diagnosing and rightly treating a mental health condition. As with the medical profession, the usual practice in the psychological field is to conduct an assessment and determine a mental health diagnosis or a provisional one (American Psychological Association, 2023). This helps determine a clear treatment plan, including identifying the appropriate intervention(s).
Part 2: Describing Social Transition
The Definition of a Psychological Intervention
First, it should be noted that social transition falls within the definition of a clinical intervention. According to the American Psychological Association, “an intervention is an ‘action on the part of a psychotherapist to deal with the issues and problems of a client. The selection of the intervention is guided by the nature of the problem, the orientation of the therapist, the setting, and the willingness and ability of the client to proceed with the treatment’” (American Psychological Association, 2023). Arnberg et al. (2013) described the intervention as a method to improve health by means of strategies that induce changes in a patient's cognitions, emotions, and behaviors, according to an explicit psychological theory. There are three key features to a psychological intervention: 1) it is employed by the psychotherapist; 2) it is done to improve health; and 3) the results are dependent on the willingness of the client to proceed with treatment (American Psychological Association, 2023).
Regarding the nature of social transition, two systematic reviews noted, “even though social transition is undertaken outside healthcare settings, it is important to view [social transition] as an active intervention because it may have significant effects on the child or young person in terms of their psychological functioning and longer-term outcomes” (Cass, 2024, p. 158; Department of Health and Human Services, 2025b). These reviews are in keeping with one of the foremost experts on gender dysphoria. Almost ten years ago, Kenneth Zucker (2018) remarked, those who “support, implement, and encourage a gender social transition are implementing a psychosocial treatment that will increase the odds of long-term persistence.”
The Use of the Social Transition
What is social transition intervention? Social transition is part of the gender affirming care model (GAC), and it continues to be the primary intervention associated with gender dysphoria. While the model is not necessarily applied in an entirely linear fashion, the typical first step in this intervention is social support or the social transition (WPATH, n.d.). This step is supposed to be the least physiologically invasive part of the bigger model, which has been suggested by WPATH for children and adults alike. The purpose of the intervention has been described as a means for reducing psychological distress and preventing suicide (“life-saving care,” as it is commonly described) (WPATH, n.d.).
The World Professional Association for Transgender Health’s (WPATH) standards of care (version 8) defines the social transition intervention through the following: 1) adopting a change that might include their name, pronouns, identification (e.g., birth certificate, identification cards, passport, school and medical documentation); 2) their participation in sex-segregated programs and spaces; 3) changing their hair and clothing style; and 4) communicating one’s preferred gender to others.
The WPATH guidelines also suggest that children as young as 18 months can have an awareness of their gender and benefit from support to use a different name, hairstyle, and clothing that aligns with their preferred gender (Coleman et al., 2022). WPATH sees the social transition step as one means to decide if a person needs gender affirming surgery (2022).
Gender Affirming Care Model and Intended Outcomes
As previously stated, an unclear or poorly devised diagnosis and assessment can lead to difficulties with creating accurate treatment goals. In other words, it is difficult to understand what needs to be changed when the prescription is ambiguous. This fact is demonstrated in the GAC objectives. The figure below illustrates what the GAC intervention model claims to do. As depicted in Figure 1, the goals and expected outcomes for GAC follow left to right.
Figure 1
Expected Outcomes from Gender Affirming Care
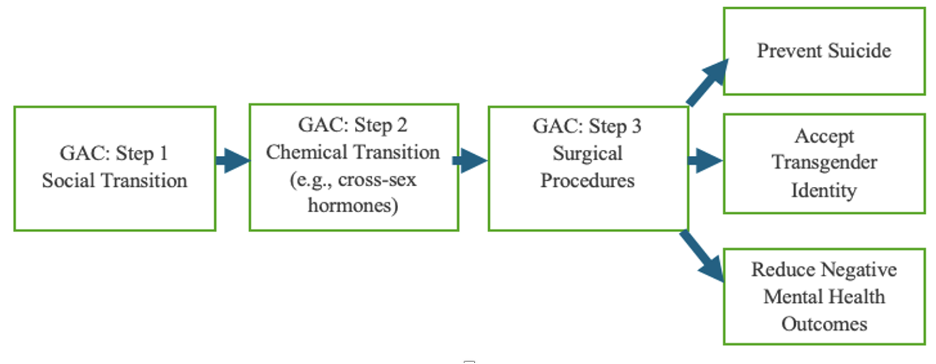
The goals of the GAC model have been outlined in the WAPTH guidelines (Coleman et al., 2022), have been promoted by government health services nationwide (Assistant Secretary for Health, 2022), and are a part of the scientific discourse (e.g., Endocrine Society, 2024). The goals include preventing suicide, lowering negative mental health symptoms, and helping a person embrace a transgender identity (Green et al., 2022; Goetz & Arcomano, 2023). The primary basis for these outcomes is driven by the theory that psychological distress is associated with being a part of a minority group (Sutter & Perrin, 2016). In this way, affirmation and support are thought to reduce negative psychological symptoms, including suicide.
Reviews of the Literature Addressing Social Transition & GAC
Despite the lack of empirical evidence, the social transition step in the gender affirming process has been the most widely applied by clinicians, paraprofessionals, and school officials alike.
To date, the research on the gender affirming care intervention has primarily focused on physiological procedures, including the use of puberty blockers, cross-sex hormones, and surgical procedures. There is very little data available on the first step of the GAC model. National and international governmental health services have conducted systematic reviews of the GAC model (e.g., Council for Choices Healthcare Finland, 2020; Department of Health and Human Services, 2025b; National Institute for Health and Care Excellence, 2020). The findings from the two most recent reviews included social transition, and the results showed that the effects were low or absent on negative mental health outcomes (Department of Health and Human Services, 2025b; Cass, 2024).
Despite the lack of empirical evidence (Morandini et al., 2023), the social transition step in the gender affirming process has been the most widely applied by clinicians, paraprofessionals, and school officials alike (Land, 2023; Foust, 2022). While it is the easiest and most accessible step to implement, it is an intervention that has potentially “significant effects” (Department of Health and Human Services, 2025b; Cass, 2024).
Studies have repeatedly found that children who are given basic support and/or are left alone (without intervention) to resolve distress about their biology mostly come to embrace their natal sex at a rate that ranges from 65-94%.
Studies have repeatedly found that children who are given basic support and/or are left alone (without intervention) to resolve distress about their biology mostly come to embrace their natal sex at a rate that ranges from 65-94% (Brooks, 2018; Rawee et al., 2024; Ristori & Steemsma, 2016; Singh et al., 2021). This means that there is a 65% to 94% success rate when no intervention or a supportive model is applied. In other words, not only does non-intervention have a better success rate than the GAC model, but it is also more successful than most psychological interventions associated with a DSM diagnosis, which, statistically, show small effect sizes and seem to be subject to ceiling effects (Leichsenring et al., 2022). Unfortunately, those who are encouraged to socially transition tend to progress to the more dangerous and physiological aspects of the GAC model (e.g., cross-sex hormones, surgeries) and may still suffer from dysphoric symptoms (e.g., Sweden, Finland, England, Denmark, U.S.).
Emerging Outcomes and the Gender Affirming Care Model
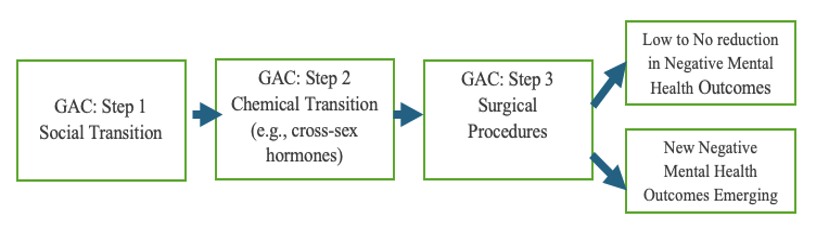
Below, Figure 2 depicts the outcomes that reportedly result from the GAC treatment model. The caveat is that negative mental health outcomes are only beginning to emerge in the literature. Some of these investigations have examined those who end GAC or attempt to reverse the social, chemical, and/or surgical procedures initiated by the intervention (Irwig, 2022; Kettula et al., 2025). The initial findings from this new body of literature reveal that patients are reporting regret from every stage of GAC (Kettula et al., 2022). The full effects of this are yet to be seen.
Figure 2
Results from Systematic Reviews of Gender Affirming Care and Emerging Outcomes
Developmental Considerations
In addition to the reviews of the literature and research on regret, developmental psychology can also shed light on reasons why socially transitioning a minor should garner the utmost caution from the clinical and scientific community. In the early years of a child’s life, their sense of self is still taking shape and remains particularly sensitive to adult feedback and to the social environment more broadly (Harter, 2012). Decades of cognitive research show that children in the preoperational and concrete-operational stages think in immediate, concrete terms and lack the capacity to reason through long-range implications (Siegler et al., 2020). This research has since been confirmed using f-MRI technology to scan the brain. The results show that some of the most important neurological strides pertaining to emotional and cognitive development are not achieved until most people are in their twenties (Nadig, Seidlitz, McDermott, Raznahan, et al., 2021). This research reveals that children do not have the capacity to understand the long-term implications of the interventions that are reshaping their identity.
Decades of cognitive research show that children in the preoperational and concrete-operational stages think in immediate, concrete terms and lack the capacity to reason through long-range implications.
Early research on children's suggestibility adds another layer: adult cues influence not just what children report but how they come to understand themselves (Bruck & Ceci, 1999). When a child adopts a new name, pronouns, and social role, the adults around that child inevitably respond in ways that reinforce the new identity. That kind of shift is not a neutral reflection of inner certainty. The National Health Service-commissioned Cass Review explicitly characterized social transition as “an active intervention” with potentially “significant effects on…psychological functioning” (Cass, 2024, p. 158). Social transition is an intervention in the child's developmental environment at a point when identity is still highly unsettled.
Etiological and Comorbid Factors
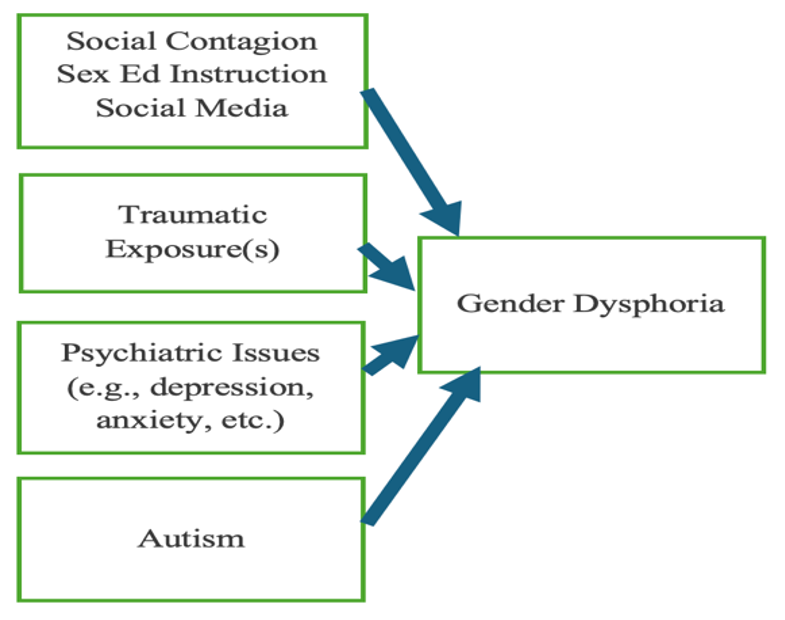
The GAC model does not adequately consider other potentially potent etiological or comorbid factors that might best account for the symptoms of gender dysphoria (see Figure 3a; Littman, 2018). Some of these factors might include traumatic experiences (Meyer et al., 2021), psychiatric issues (Frew et al., 2021), and autism (Van Der Miesen et al., 2016). This area of research has been neglected despite a general awareness of these social, psychiatric, and medical factors (e.g., The Trevor Project, 2020).
Figure 3a
Known Comorbid Factors
Known Factors and Proposed Outcomes
Taken together, Figure 3b shows what should follow a determination of gender dysphoria. This image illustrates a treatment goal and intervention that matches the psychological nature of the problem of gender dysphoria with an aim to reduce the dysphoria and psychological distress and bring the person’s psychology into alignment with their biology.
Figure 3b
A Model for Treating Gender Dysphoria and Related Comorbidities and the Expected Outcomes
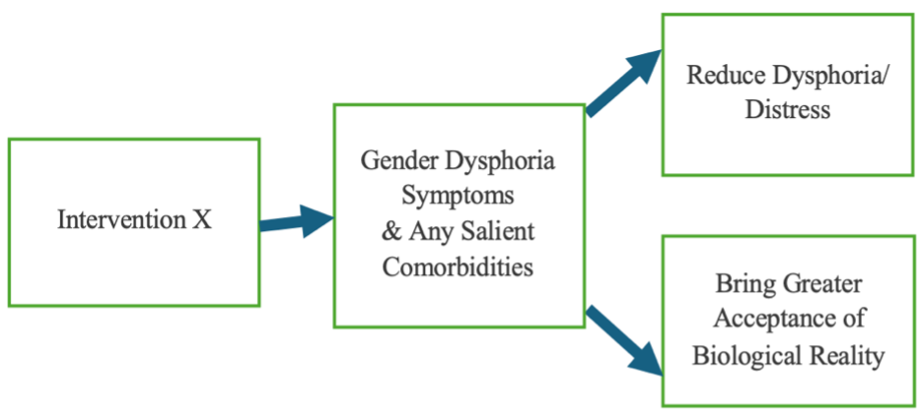
As depicted in Figure 3b, intervention X (which does not exist yet) is mostly absent from the scientific discourse and from the practice setting. This figure highlights the need for new research and other interventions to be constructed to properly address psychological distress, reduce dysphoria, and bring a person’s psychology into alignment with their biological sex.
Currently, there is only one alternative to the gender affirming care model that has been discussed in scientific literature: watchful waiting (de Vries & Cohen-Kettenis, 2012). Watchful waiting has not been promoted by advocates of GAC or professional groups (e.g., American Academy of Pediatrics; American Psychological Association; Anxiety & Depression Association of America). It was also used primarily with prepubescent minors. As a new cohort of gender dysphoric youth have emerged, the research has not kept pace in understanding their unique challenges. To date, most of the intervention research has focused on the gender affirming care model (Keo-Meier & Ehrensaft, 2018), which advocates for grand physiological and psychological disruptions. However, national reviews of the literature are now promoting talk therapy over GAC (e.g., UK; U.S.).
In review of the efficacy of social transition, it should be noted that while social transition has been mostly characterized as a psychological and behavioral intervention, there is growing concern that aspects of social transition are causing physiological harm (Bumphenkiatikul et al., 2025, p. 5). In fact, in a study conducted by the Department of Health and Human Services, one reviewer noted that parts of social transition should also be considered as physiological interventions because of the potential damage that can occur to the body (Department of Health and Human Services, 2025a). This can be seen when a female who wants to appear as a male is encouraged to use a breast binder to flatten her chest. A male who wants to appear as a female may be encouraged to tuck his penis and scrotum to hide his genitalia. As written in the HHS report, “a significant number of negative health implications have been reported [for chest binding], with rates as high as 97.2%” (Bumphenkiatikul et al., 2025, p. 5), noting that social transition is not without physiological consequences.
Part 3: Addressing the Use of Social Transition by Clinical and Non-Clinical Individuals
Social Transition Intervention Should Not Be Used to Treat Gender Dysphoria
There are two groups that most often apply the social transition intervention to children. First, there are mental health professionals who are credentialed and, therefore, are allowed to use psychological interventions. While this is the appropriate group to employ an intervention, these professionals should stop applying social transition based on reviews of the currently available literature which do not lend support to any part of the GAC model. Further, the literature demonstrates that the risks outweigh the benefits of treatment and offers no other path for health in both mind and body.
Additionally, clinicians should not use the intervention because of the numerous study questions that have not been asked about social transition, like, “What are the long-term psychological and sociological effects of engaging in social transition?” This question has serious implications for the developing minor and the coherence of his or her identity. Additionally, there is a lack of understanding about if and how known comorbidities contribute to gender dysphoria (e.g., Frew et al., 2021; Kallitsounaki & Williams, 2023). As previously mentioned, there is some evidence that shows how the practices surrounding social transition can be physiologically damaging, but this, too, has not been thoroughly evaluated (Hall et al., 2024).
No Paraprofessional, School Employee, or Individual Should Use Social Transition
The second group commonly using social transition—but without clinical credentials—are educators, school employees, and paraprofessionals. Just as no mental health professional should use the social transition intervention on the basis of weak evidence, no one else should use the intervention either.
As mentioned in the literature review, the confusion that surrounds a diagnosis of gender dysphoria has led to poorly crafted treatment assessment and goals. Although the potential ramifications of the social transition intervention are significant (Zucker, 2018), such practice can be easily applied by anyone. This fact, combined with the lack of enforcement around the treatment protocol, has resulted in widespread and non-clinical use of a psychological intervention intended to treat the disorder of gender dysphoria.
Despite this fact, social transition intervention has been instituted by schools across the country. This can be readily seen in what has been referred to as the gender closets, which have been funded by various groups, where children can change into the opposite sex’s clothing while they are at school and do so without their parents’ or caregiver’s knowledge (e.g., California, New Mexico, Washington, Texas). The educational system has also been used to promulgate the ideas that describe gender dysphoria. This is seen in school curricula, libraries, and social media platforms. Reading lists (Early Childhood: Learning about Gender Identity, n.d.) with books (Giddings, 2022) like Gender Queer and I Am Jazz are read in classrooms and are stocked in libraries with the aim to introduce and normalize the ideas of the gender dysphoria construct to children. Furthermore, curricula (Welcoming Schools, n.d.) and resources (Glisten, 2026) for teaching elementary school children about the transgender experience have also been instituted in classrooms. All of this has been done without any empirical data on the long-term effects of introducing children to these concepts or the outcomes of implementing the social transition model with or without parental consent.
Policy Recommendations
To date, only a handful of states have passed bills to protect children from the deleterious effects of social transition, including South Carolina, Tennessee, and Texas. Conversely, California passed AB 1955 (2024) to prohibit parental notification for a child who is taking steps towards a social or physiological transition.
In 2023, Montana passed one of the most comprehensive bills that prohibited clinicians, school officials, and paraprofessionals from attempting to socially transition a child (SB 99), but it has been permanently enjoined by the state Supreme Court in a suit brought by the ACLU. Subsequently, Texas passed important legislation targeting social transition (SB 12, 2025; SB 113, 2025). Below are policy recommendations that states and the Trump Administration can take to advance protections for minors subject to the unscientifically supported use of social transition.[1]
Mental Health Clinicians
- Medical and mental health professionals should not be involved in the social transitioning of a minor. States should direct clinical licensing boards to investigate claims of clinicians engaging in this dangerous practice, with the potential of licensing revocation and financial penalties.
- States should create reporting requirements for state licensing boards to track complaints related to gender dysphoria treatment in minors.
- Federal guidance from the U.S. Health and Human Services (HHS) should establish that initiating social transition without adequate assessment of comorbid conditions (e.g., trauma, autism, other psychiatric conditions) violates professional standards.
- States should direct licensing and accreditation boards to remove training, education, and continuing education credits for units that promote gender affirming care. State accrediting bodies should not grant institutions of higher education accreditation if they provide courses that promote gender affirming care. Instead, the experiences of detransitioners and the harms of gender affirming care should be recognized in education requirements in the mental health profession.
- States should codify that social transition constitutes a psychological intervention and is therefore subject to informed consent and standard-of-care obligations.
Schools and Paraprofessionals
- Because social transition is a psychological intervention, prohibit non-licensed school personnel from initiating or facilitating it—including the use of names, pronouns, or gender expressions inconsistent with biological sex—without written parental consent (see Texas’s SB 12).
- Both state and district level policies should prohibit teachers, paraprofessionals, counselors, and other staff from providing instruction, material, information, or resources to minors about social transition.
- States should require school counselors to operate within the scope of licensure and refer gender distress to licensed mental health professionals.
- Prohibit schools from maintaining policies that conceal information about a student's psychological status, identity, or behavior from parents.
- Prohibit school resources from being used to provide materials promoting social transition (e.g., “gender closets”).
Parental Consent and Protection
- Ensure that anyone tasked with caring for a minor must immediately inform the child’s parents of the minor’s intent or desire to socially transition.
- Provide a path for civil causes of action which would allow for compensatory damages, attorney’s fees, court costs, and psychological and physiological damages that resulted from social transitioning a minor.
- States should ensure the curriculum is free from gender ideology.
- Require written, opt-in parental consent before any psychological intervention, screening, or assessment is administered to a student—including social transition and assessments embedded in classroom exercises (see Texas’s SB 113; Tennessee Code 49-2-124).
- Prohibit schools from using a parent's refusal to consent as grounds for reporting neglect or any adverse action against the student.
- Create a presumption of harm when a psychological intervention, including social transition, is initiated without parental consent, thereby shifting the burden to the defendant in civil proceedings.
The aforementioned policy recommendations will provide children and parents protection against the dangerous practice of social transition. These protections are necessary, but do not address the unanswered research questions noted in the latest systematic reviews conducted by HHS (2025a) and NHS (Cass, 2024). To better understand the needs of children presenting with distress about their biological sex, future research should consider investigating the topics below.
Research Considerations
- National Institutes for Health and the Office of the Assistant Secretary for Health (HHS) should prioritize research into etiology, including comorbid conditions, trauma, and autism spectrum disorder.
- National Institutes for Health and the Office of the Assistant Secretary for Health (HHS) should support the development of therapeutic approaches that aim to resolve dysphoria and align psychological well-being with biological reality.
[1] For other actions states can take to combat gender ideology in K-12 schools, see Schorr, 2025.
Resources